



Articles
Who doesn’t love these adorable frenchies?! French bulldogs have become increasingly popular with their small size and distinct appearance. Unfortunately, what makes these dogs incredibly cute can also lead to a variety of health issues. As veterinarians, it’s important to recognize the issues that affect these dogs and understand when specialty care may be beneficial to ensure the best outcome. In this article we will focus on common neurological conditions affecting the breed.
- Intervertebral disc disease (IVDD)
This is one of the most common neurologic conditions affecting the French bulldog, in particular due to Hansen type 1 disc extrusions. Their chondrodystrophic anatomy predisposes them to premature disc mineralization. They generally occur in dogs of 2 years plus.
Signs: Dogs may present ranging from pain only (cervical or thoracolumbar) to complete paralysis (tetra or paraplegia). Depending on the location of the injury, fecal and or urinary continence may be present.
When to refer: Any dog that has lost the ability to walk, is exhibiting severe discomfort non-responsive to medical management or any dog that is unable to feel his toes.
Recommendations and approximate cost: Advanced imaging (MRI preferred) and potentially decompressive surgery (ventral slot or hemilaminectomy). Average cost for imaging and routine decompression is $9000-12000. Cost depends on the pet’s neurologic status at time of diagnosis.
- Hemivertebrae and congenital malformations
Congenital spinal abnormalities including hemivertebrae and subarachnoid diverticulums are extremely common among the breed. In fact, over 80% of French bulldogs suffer from hemivertebrae. Hemivertebrae are often incidental findings so no need to panic if found on thoracic radiographs in a neurologically normal pet. The severity of the malformation does not necessarily correlate with the severity of spinal cord compression. Subarachnoid diverticulum can be more problematic. SIgns may present from a very early age.
Signs: Generally, these dogs are minimally painful, and the onset of weakness is more gradual. More commonly affects the thoracolumbar spine, however, malformations of the cervical spine are possible.
When to refer: Any dog that has progressive weakness with radiographic changes concerning for congenital malformations. Some can be successfully managed with steroids and physical therapy. Any owners that wish to obtain a definitive diagnosis as this will necessitate advanced imaging such as an MRI.
Recommendations and approximate cost: Advanced imaging (MRI preferred) and potentially decompressive surgery (subarachnoid diverticulums). Average cost for imaging alone is $3500-4500 and imaging and decompression is $9000-11500. Some cases require advanced stabilization techniques and estimates can be provided on a case-by-case basis.
- Meningoencephalitis and Brain tumors
French bulldogs are also prone to intracranial disease. Meningoencephalitis and intracranial neoplasia may present in similar ways. While immune mediated meningoencephalitis is more common in young dogs, French bulldogs are prone to brain tumors such as gliomas which can present in a younger population and typically carry a poorer prognosis.
Signs: Behavior changes, vestibular disease, circling, unexplained pain and seizures. These dogs are typically sick and early signs may include lethargy, nausea, and mentation changes.
When to refer: Any dog that has concern for intracranial disease, early diagnosis may lead to better outcomes especially with meningoencephalitis. These dogs can go downhill rapidly so if no clear cause can be determined on exam it is always best to refer these patients.
Recommendations and approximate cost: Advanced imaging (MRI) +- spinal tap. Average cost for imaging alone is $3500-4500. Some cases may require prolonged hospitalization and intravenous cytarabine for best outcome (meningoencephalitis). Infectious disease testing may also be recommended depending on the pet’s history. Cost may vary depending on how sick the patient is. Stereotactic radiation is the current best recommendation for gliomas and referral can be provided if elected.
- Epilepsy
French bulldogs are also very prone to generalized seizures. They key to differentiating these dogs from dogs with structural intracranial disease is that dogs with primary epilepsy are normal in between seizures. Given the predilection for meningoencephalitis, a workup to include MRI and spinal tap is generally recommended early on to ensure there is no underlying disease.
Signs: Recurrent seizures may vary from focal to generalized seizures. Focal seizures are more likely to be secondary to structural disease.
When to refer: Any dog that has concern for intracranial disease, early diagnosis may lead to better outcomes. Seizures that are difficult to control or pets with multiple comorbidities necessitating close monitoring.
Recommendations and approximate cost: Advanced imaging (MRI) +- spinal tap. Average cost is $3500-4500.
Key considerations when considering referral:
In many cases, early intervention can significantly improve the pet’s prognosis. Generally, consider referral if you observe any of the following:
- Sudden or gradual inability to walk.
- Severe or unmanageable pain
- New or persistent seizure activity
- Breathing related issues in brachycephalic dogs
- Any case where the pet’s owner seeks a definitive diagnosis and therefore requires advanced imaging.
Conclusion
Neurologic diseases can range from mild to life threatening in French Bulldogs. Early diagnosis can help improve long-term outcome. As veterinarians it is our responsibility to recognize these diseases and when referral may benefit these patients. Working together helps us provide the best possible care for these pets and increases the treatment options available so that as a team we can improve the quality of life for these little gremlins! The popularity of the French bulldog is here to stay and here at MVA we look forward to helping you and their owners provide the best care for the best possible outcome. Please note, these are routine estimates, as cute as these guys are, we all know these cases are not always routine! These prices are accurate at the time of writing.
Select Surgical Diseases of the French Bulldog
The French Bulldog has risen in popularity over the last several years, displacing Labradors from the top place in 2022 after a 31-year reign on the AKC published most popular breeds table. This is a cause for concern for veterinarians as the breed conformation extremes of the French Bulldog predispose them to numerous health concerns. A study published in the UK surveyed presenting complaints for 2,781 French Bulldogs and 21,850 non-French Bulldogs at primary care clinics. They found, the French Bulldog had significantly higher risk for 20/43 (46.5%) of the studied common disorders compared to non-French Bulldogs.1 This article will briefly discuss three potentially surgical disorders that commonly occur in the breed and how to decide when surgery is indicated.
Brachycephalic Obstructive Airway Syndrome (BOAS)
Brachycephalic Obstructive Airway Syndrome is an umbrella term for structural abnormalities, due primarily to conformation, that leads to obstruction of airflow in brachycephalic dogs. French Bulldogs are reported to have a 31-fold increased risk of BOAS and in particular 42-fold increased risk of stenotic nares compared to the general population.1
The components associated with BOAS can be considered primary (anatomic abnormalities the dog is born with or develops during growth) and secondary (changes that develop as a result of the primary changes). The primary abnormalities include stenotic nares, nasopharyngeal turbinates, and hypoplastic trachea. An elongated soft palate can be both a primary and a secondary abnormality.
Poiseuille’s law states that the radius is inversely related to resistance to the power of 4, or in other words, a 50% reduction in the airway radius will lead to 16 times increase in airway resistance. At each primary abnormality, the passage for airflow is narrowed causing increased airway resistance and turbulence. The increased negative pressure created by the animal to overcome the resistance leads to inflammation of the soft tissue and the appearance of secondary changes such as everted tonsils, everted laryngeal saccules, laryngeal collapse, and edema of the pharyngeal tissue further compounding the issue.
Laryngeal collapse is the result of chronic increased negative pressure causing cartilage weakening. There are three stages, the first is everted laryngeal saccules which are reported in 53-66% of BOAS cases. The second stage is the loss of rigidity and medial collapse of the cuneiform processes of the arytenoid cartilages, and stage III is the medial collapse of the corniculate processes.
Diagnosis of BOAS is based on history and physical exam. Although respiratory signs such as stertorous breathing, exercise and stress intolerance, and dyspnea are primarily associated with BOAS, there are other clinical signs as well such as sleep disorders, GI signs, and urethral prolapse that can be improved with addressing the upper airway obstruction. A group in the UK validated an exercise tolerance test and grading system to help with the diagnosis of BOAS in brachycephalic breeds to help guide surgical decisions and breeding. For this test, they assessed dogs at rest and then after a moderate trot (3-5mph) for 3 minutes and graded the presence of airway noise and effort (table 1).2 For dogs that already showed moderate to severe signs (grade III) at rest, the trot test was not required. They found the inclusion of a 3-minute trot test increased the sensitivity of diagnosing BOAS to 93%, compared to 57% on pre-exercise tolerance test.2 Additionally, they found the presence of stridor on exam to be 100% specific for laryngeal collapse.2 Based on this scheme they proposed a treatment plan, for dogs under two years old with grade 0-1 disease, that are clinically unaffected, annual health checks can be performed for progression of disease. For grades 2 and 3, these dogs would benefit from veterinary treatment, which often consists of a combination of medical and surgical management. They also made the recommendation for grade 3 dogs to not be bred and breeding of grade 2 dogs to only be to dogs that are grade 0-1.2,3
It is important for owners to understand that surgery is part of the management but will not give dogs a normal airway. Owners should be counseled to be cautious of heavy activity, especially in hot and humid weather, and to use a harness for walking. When surgery is performed early in life (<2 years) prior to secondary changes, these dogs will often live a normal life. However, in a long-term study of 62 dogs that underwent surgical correction, the treatment success rate was 94.2% and the outcome was not affected by age, therefore surgery should be considered as an option in all dogs. In dogs with stage II or III laryngeal collapse, the prognosis is guarded.
Complications include laryngeal swelling that may cause respiratory distress and necessitate a temporary tracheostomy, regurgitation or vomiting, and aspiration pneumonia. In dogs where not enough palate is resected, the clinical signs can continue, and dogs who have had too much palate resected may experience intranasal reflux. There is a potential for laryngeal webbing to develop following laryngeal sacculectomy or with accidental iatrogenic trauma to the larynx. In a large study of 248 brachycephalic dogs undergoing airway surgery, the peri-operative mortality rate was 2.4%.19
There are two main categories for soft palate reduction, a staphalectomy which purely shortens the palate, and a palatoplasty which shortens and thins the palate. As many brachycephalic breeds have both an overlong and overly thick palate, palatoplasties are becoming more popular.
Staphalectomy can be performed with CO2 laser, ligasure, or with a cut and suture method. Similar outcomes are generally reported between the three methods. The palate is generally resected to the level of the mid palatine tonsils. In contrast, the folded flap palatoplasty is performed by resecting the ventral mucosa along with the palatinus muscle and part of the Levator Vili. The caudal tip of the palate it then folded forward and sutured to the rostal aspect of the resected area.
One of the most widely performed techniques to widen the nostrils is the vertical wedge. A vertical wedge in the wing of the nostril is planned depending on the amount of tissue you wish to remove. Once the wedge is removed, the area is closed with 3-0 or 4-0 suture material effectively lateralizing the medial edge of each alar wing. An alternative procedure that is gaining popularity for providing more open naris is the ala-vestibuloplasty. In this procedure, the vestibular fold and the alar wing are both amputated. Bleeding is controlled with direct pressure and topical epinephrine and the wound edges are left to heal by second intension. The benefit of this procedure over the wedge is it allows for deeper opening of the nasal passage by ways of addressing both the alar wing and the vestibular fold (fig.1). Recently, a study was published comparing the opening of the nares between the standard vertical wedge and the ala-vestibuloplasty. This study performed the two procedures along with a modified wedge on 3D printed replicas of a single French Bulldogs nose. The ala-vestibuloplasty provided significantly greater cross sectional widening than the other procedures. However, no clinical studies directly comparing ala-vestbuloplasty to the wedge resection have been performed.20
Otitis
French Bulldogs are reported to have a 14-fold increased risk of presenting with ear discharge than the general population.1 In an anatomic CT study of French Bulldogs (n=55) and pugs (n=20), the brachycephalic breeds had a significantly higher incidence of narrowed external ear canal’s (82.6%) and middle ear effusion (44%).4 Another study looking at the influence of extreme brachycephalic conformation in dogs undergoing total ear canal ablation and lateral bulla osteotomy (TECA-LBO), found these breeds commonly presented at a younger age and more oto-neurologic signs such as facial nerve paralysis, vestibular syndrome, and Horner’s syndrome compared to other breeds.5
Although most ear disease can be managed medically, surgery is recommended for dogs with end-stage ear disease, the presence of masses, dogs that are refractory to appropriate medical management, and when discomfort from ear disease is affecting quality of life despite appropriate medical management. End stage ear disease refers to complete stenosis of the ear due to proliferation and calcification of the external ear canal secondary to chronic ear inflammation. With severe stenosis, the ear canal is no longer able to naturally drain and from a treatment standpoint it is no longer accessible by topical medications.
The recommended surgery is a TECA-LBO which refers to the surgical excision of the entire external ear canal combined with removal of the lateral wall of the bulla to allow middle ear debridement. It is important all of the ear canal and lining of the middle ear is removed to prevent post-operative draining tracts. Prior to surgery, a CT is often recommended. In brachycephalic breeds a higher incidence of bilateral changes, aural masses, para-aural abscesses, otitis externa, and brainstem changes are reported compared to non-brachycephalic breeds.5
TECA-LBO surgery does have some potential complications. The most common intra-operative complication is severe hemorrhage from one of the neighboring vessles.6 Severe hemorrhage requiring transfusion is reported in 5.5-15.6% of cases.7,8 The most common post operative complications include wound related complications (2-50%), facial nerve paresis or paralysis (13-36%), vestibular disease (1-8%), and Horner’s disease (1-8%).9-12 Some hearing loss is also expected, however, the degree of additional loss has been questioned for dogs with preexisting end stage disease, as often the dog’s hearing is already compromised. Despite the conformation specific findings and increase in technical difficulty to perform a TECA-LBO in brachycephalic breeds, the complication rate is not statistically different from the general population.5
Humeral Fracture
French Bulldogs one of the breeds reported to have a predisposition to distal humeral condylar fractures. Dogs are most commonly affected while they are skeletally immature, with a peak at four months, or as an adult with the presence of an intracondylar fissure.13
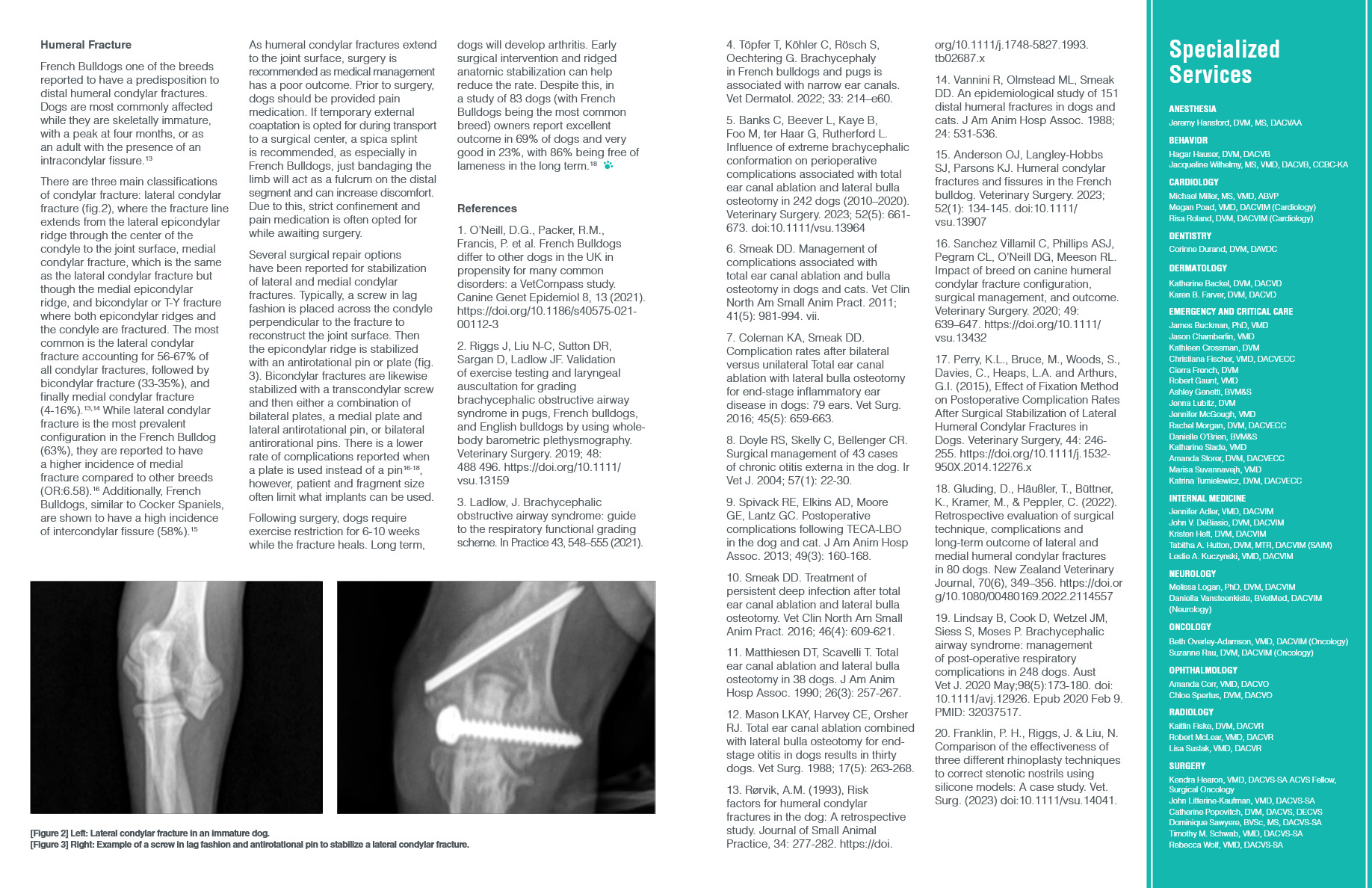
There are three main classifications of condylar fracture: lateral condylar fracture (fig.2), where the fracture line extends from the lateral epicondylar ridge through the center of the condyle to the joint surface, medial condylar fracture, which is the same as the lateral condylar fracture but though the medial epicondylar ridge, and bicondylar or T-Y fracture where both epicondylar ridges and the condyle are fractured. The most common is the lateral condylar fracture accounting for 56-67% of all condylar fractures, followed by bicondylar fracture (33-35%), and finally medial condylar fracture (4-16%).13,14 While lateral condylar fracture is the most prevalent configuration in the French Bulldog (63%), they are reported to have a higher incidence of medial fracture compared to other breeds (OR:6.58).16 Additionally, French Bulldogs, similar to Cocker Spaniels, are shown to have a high incidence of intercondylar fissure (58%).15
As humeral condylar fractures extend to the joint surface, surgery is recommended as medical management has a poor outcome. Prior to surgery, dogs should be provided pain medication. If temporary external coaptation is opted for during transport to a surgical center, a spica splint is recommended, as especially in French Bulldogs, just bandaging the limb will act as a fulcrum on the distal segment and can increase discomfort. Due to this, strict confinement and pain medication is often opted for while awaiting surgery.
Several surgical repair options have been reported for stabilization of lateral and medial condylar fractures. Typically, a screw in lag fashion is placed across the condyle perpendicular to the fracture to reconstruct the joint surface. Then the epicondylar ridge is stabilized with an antirotational pin or plate (fig. 3). Bicondylar fractures are likewise stabilized with a transcondylar screw and then either a combination of bilateral plates, a medial plate and lateral antirotational pin, or bilateral antirorational pins. There is a lower rate of complications reported when a plate is used instead of a pin16-18, however, patient and fragment size often limit what implants can be used.
Following surgery, dogs require exercise restriction for 6-10 weeks while the fracture heals. Long term, dogs will develop arthritis. Early surgical intervention and ridged anatomic stabilization can help reduce the rate. Despite this, in a study of 83 dogs (with French Bulldogs being the most common breed) owners report excellent outcome in 69% of dogs and very good in 23%, with 86% being free of lameness in the long term.18
References
- O’Neill, D.G., Packer, R.M., Francis, P. et al. French Bulldogs differ to other dogs in the UK in propensity for many common disorders: a VetCompass study. Canine Genet Epidemiol 8, 13 (2021). https://doi.org/10.1186/s40575-021-00112-3
- Riggs J, Liu N-C, Sutton DR, Sargan D, Ladlow JF. Validation of exercise testing and laryngeal auscultation for grading brachycephalic obstructive airway syndrome in pugs, French bulldogs, and English bulldogs by using whole-body barometric plethysmography. Veterinary Surgery. 2019; 48: 488 496. https://doi.org/10.1111/vsu.13159
- Ladlow, J. Brachycephalic obstructive airway syndrome: guide to the respiratory functional grading scheme. In Practice 43, 548–555 (2021).
- Töpfer T, Köhler C, Rösch S, Oechtering G. Brachycephaly in French bulldogs and pugs is associated with narrow ear canals. Vet Dermatol. 2022; 33: 214–e60.
- Banks C, Beever L, Kaye B, Foo M, ter Haar G, Rutherford L. Influence of extreme brachycephalic conformation on perioperative complications associated with total ear canal ablation and lateral bulla osteotomy in 242 dogs (2010–2020). Veterinary Surgery. 2023; 52(5): 661-673. doi:10.1111/vsu.13964
- Smeak DD. Management of complications associated with total ear canal ablation and bulla osteotomy in dogs and cats. Vet Clin North Am Small Anim Pract. 2011; 41(5): 981-994. vii.
- Coleman KA, Smeak DD. Complication rates after bilateral versus unilateral Total ear canal ablation with lateral bulla osteotomy for end-stage inflammatory ear disease in dogs: 79 ears. Vet Surg. 2016; 45(5): 659-663.
- Doyle RS, Skelly C, Bellenger CR. Surgical management of 43 cases of chronic otitis externa in the dog. Ir Vet J. 2004; 57(1): 22-30.
- Spivack RE, Elkins AD, Moore GE, Lantz GC. Postoperative complications following TECA-LBO in the dog and cat. J Am Anim Hosp Assoc. 2013; 49(3): 160-168.
- Smeak DD. Treatment of persistent deep infection after total ear canal ablation and lateral bulla osteotomy. Vet Clin North Am Small Anim Pract. 2016; 46(4): 609-621.
- Matthiesen DT, Scavelli T. Total ear canal ablation and lateral bulla osteotomy in 38 dogs. J Am Anim Hosp Assoc. 1990; 26(3): 257-267.
- Mason LKAY, Harvey CE, Orsher RJ. Total ear canal ablation combined with lateral bulla osteotomy for end-stage otitis in dogs results in thirty dogs. Vet Surg. 1988; 17(5): 263-268.
- Rørvik, A.M. (1993), Risk factors for humeral condylar fractures in the dog: A retrospective study. Journal of Small Animal Practice, 34: 277-282. https://doi.org/10.1111/j.1748-5827.1993.tb02687.x
- Vannini R, Olmstead ML, Smeak DD. An epidemiological study of 151 distal humeral fractures in dogs and cats. J Am Anim Hosp Assoc. 1988; 24: 531-536.
- Anderson OJ, Langley-Hobbs SJ, Parsons KJ. Humeral condylar fractures and fissures in the French bulldog. Veterinary Surgery. 2023; 52(1): 134-145. doi:10.1111/vsu.13907
- Sanchez Villamil C, Phillips ASJ, Pegram CL, O’Neill DG, Meeson RL. Impact of breed on canine humeral condylar fracture configuration, surgical management, and outcome. Veterinary Surgery. 2020; 49: 639–647. https://doi.org/10.1111/vsu.13432
- Perry, K.L., Bruce, M., Woods, S., Davies, C., Heaps, L.A. and Arthurs, G.I. (2015), Effect of Fixation Method on Postoperative Complication Rates After Surgical Stabilization of Lateral Humeral Condylar Fractures in Dogs. Veterinary Surgery, 44: 246-255. https://doi.org/10.1111/j.1532-950X.2014.12276.x
- Gluding, D., Häußler, T., Büttner, K., Kramer, M., & Peppler, C. (2022). Retrospective evaluation of surgical technique, complications and long-term outcome of lateral and medial humeral condylar fractures in 80 dogs. New Zealand Veterinary Journal, 70(6), 349–356. https://doi.org/10.1080/00480169.2022.2114557
- Lindsay B, Cook D, Wetzel JM, Siess S, Moses P. Brachycephalic airway syndrome: management of post-operative respiratory complications in 248 dogs. Aust Vet J. 2020 May;98(5):173-180. doi: 10.1111/avj.12926. Epub 2020 Feb 9. PMID: 32037517.
- Franklin, P. H., Riggs, J. & Liu, N. Comparison of the effectiveness of three different rhinoplasty techniques to correct stenotic nostrils using silicone models: A case study. Vet. Surg. (2023) doi:10.1111/vsu.14041.
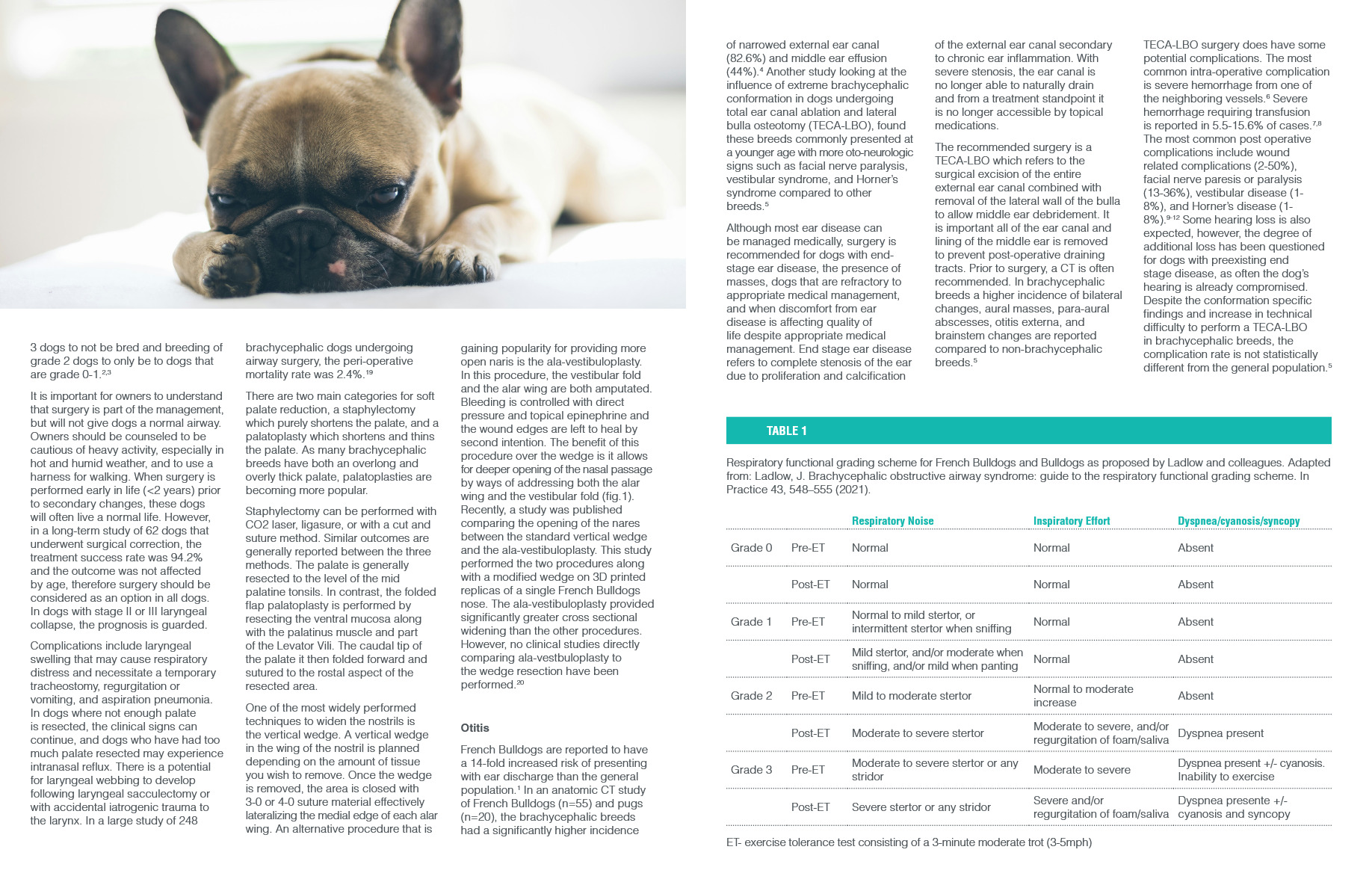
Table1: Respiratory functional grading scheme for French Bulldogs and Bulldogs as proposed by Ladlow and collogues. Adapted from: Ladlow, J. Brachycephalic obstructive airway syndrome: guide to the respiratory functional grading scheme. In Practice 43, 548–555 (2021).
| Respiratory Noise | Inspiratory Effort | Dyspnea/cyanosis/syncopy | ||
| Grade 0 | Pre-ET | Normal | Normal | Absent |
| Post-ET | Normal | Normal | Absent | |
| Grade 1 | Pre-ET | Normal to mild stertor, or intermittent stertor when sniffing | Normal | Absent |
| Post-ET | Mild stertor, and/or moderate when sniffing, and/or mild when panting | Normal | Absent | |
| Grade 2 | Pre-ET | Mild to moderate stertor | Normal to moderate increase | Absent |
| Post-ET | Moderate to severe stertor | Moderate to severe, and/or regurgitation of foam/saliva | Dyspnea present | |
| Grade 3 | Pre-ET | Moderate to severe stertor or any stridor | Moderate to severe | Dyspnea present +/- cyanosis. Inability to exercise |
| Post-ET | Severe stertor or any stridor | Severe and/or regurgitation of foam/saliva | Dyspnea presente +/- cyanosis and syncopy |
ET- exercise tolerance test consisting of a 3-minute moderate trot (3-5mph)